Saving an Hour a Year
According to the CMS they have “proposed historic changes to Physician Fee Schedule (PFS) and the Quality Payment Program (QPP) to restore the doctor-patient relationship and streamline clinical billing.” The funny thing is that I remembered this “blended” trick years ago and it either failed or didn’t pass. No matter as it doesn’t affect me now but it does affect MOST other doctors. You all can debate the merits of this plan. Will it make doctors go faster, see more patients and document less because they can all bill a 99212? Will they make more or less money? Who knows? What CMS did say on their site was this:
Removing unnecessary paperwork requirements through the PFS proposal would save individual clinicians an estimated 51 hours per year if 40 percent of their patients are in Medicare.
Interesting. I was fixated on this time estimate and I couldn’t figure out why. I knew I saw something like it before but where? Then it hit me…..on Facebook. Let’s bring in the clowns:

I just love when the AMA saves the day. I guess the whole EMR problem goes away by joining the AMA? Not. In fact, they agreed to every quality metric and P4P plan given to us that eventually drowned doctors in meaningless tasks. They helped start this whole mess. That being said, and if they are correct in their number, why doesn’t the AMA just tell CMS “we’ll fix the log-on problem for doctors and you leave things alone? This way no one gets hurt and we save the doctors one hour a year. And to be nice we will allow the doctors to do anything they want with that one hour……..as long it’s documented.”
Get Dr. Farrago’s book on how to start your own DPC practice here on Amazon





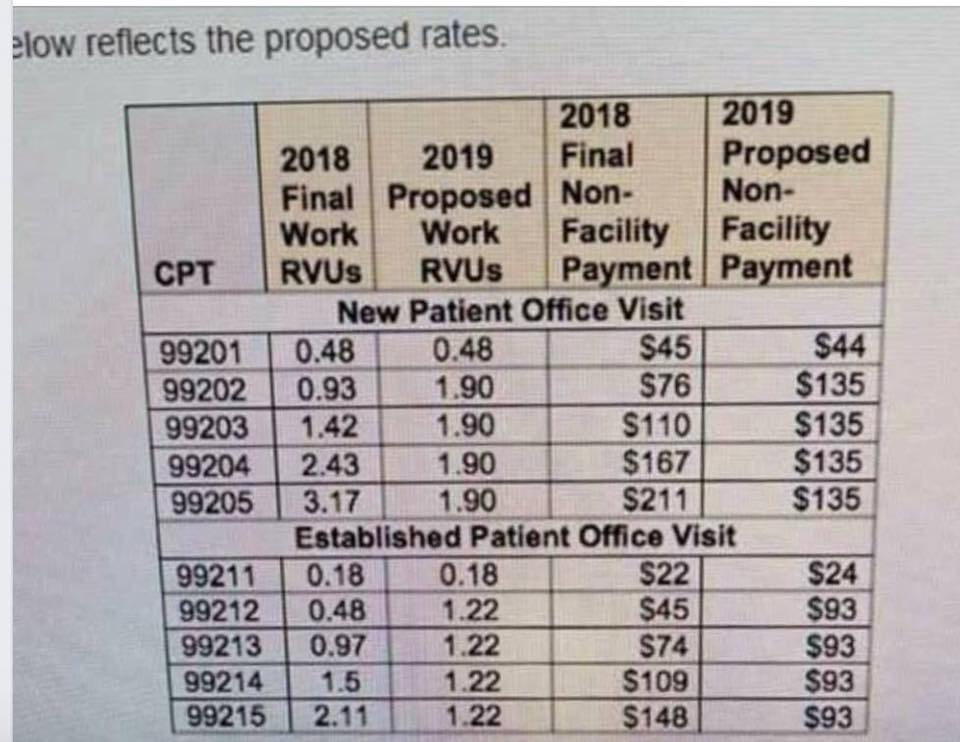
This is simply an illusion regarding not requiring documentation. You have to document everything for merit based pay. So now they don’t need to require the documentation points for EM coding. Plus it’s a great way to decrease my pay since most Medicare visits are 99214, which is now paid less. Basically I get paid less for each visit but have to document more to make my pay coefficient for merit based pay. Great scam. I have already been limiting my Medicare patients to avoid the merit based pay minimums AND to avoid being overexposed to Medicare’s ever changing payment schemes. Now I might need to say goodbye to Medicare altogether. Direct Primary Care will be the way to go. If they want me to continue seeing Medicare patients then they need to pay me well and just let me do my job. No complicated intrusive reporting mandates.
The 51 hours saved each year works out to about 12 minutes a day in the office. Enough time to use the restroom during a busy day. The new pay scale also helps to lower my income tax!
AMA stumbles from stepping on one turd- to the next. The smell is downright awful.
What is busted in this new CMS revision of billing, is the same thing that is busted in many people’s understanding of micro-economics. The price of a thing is a private value which is determined by two parties. One person decides what to pay for something that is desired. The other person will accept money in exchange for the item or service. That is the price.
There is no “objective value” to price. People may reach a common consensus of what they will offer for a thing, and call it the average retail price. That is an observation on the market, not a compelling fact. People have been accustomed to being told what the prices are.
Price-fixing, which is what CPT codes are, is the replacement of true price with an artificial value. Since markets change quickly, there is no way to mandate a price of something that matches the individual valuation of that item or service. Regulators are too slow. Therefore, shortages or gluts on the market occur.
The AMA is nuts. They have decided that half the work should be put in for a 99215 as before; but three times the work put in for a 99212. Perhaps it is a way of backing off the onerous mandates of a high-level visit, which seem to be scripted by a grammar-school student.
“Is your grandmother still dead from a heart attack?” “What was your granduncle’s shoe size?” Patients are frustrated and bewildered by the coding requirements. Patients now seem to believe that the quality of the visit is determined by the number of body parts examined, and the number of questions asked about things allergic, cardiovascular, constitutional, ears, nose, mouth, throat, endocrine, eyes, gastrointestinal, genitourinary, hematologic, immunologic, integumentary, lymphatic, musculoskeletal, neurologic, psychiatric and respiratory.
The doctor nods, and gives you a prescription. That is an office visit.
I am driven to distraction by the rubbish that has been ingrained into my patients’ expectations. “How have you been doing?” is usually followed by “What do my labs say about that?”
The next step in the tango is to criticize the patient about behavioral faults, evoking abject denials from patients. “Your A1C is 10.5%” This evokes, “Yeah, I don’t know why, all I eat is celery.” and visit, c’est fini.
Patients are confused when they come in; they are confused when they go out. They don’t value the visit; they are taught not to. They believe that a medical visit is simply the inflation of a medical chart.
If people cannot decide on the value of something, it may be worth nothing. That is the summit of achievement that American medicine has reached.
As you can see, the payment for a major complicated patient is the same as a minor ailment. Yet another reason to avoid taking care of sick people. What are these idiots thinking?