Deceit, Fraud and Chasing Money: Don’t Expect Your Professional Organizations to Help!
Last year, a well dressed representative came into our Internal Medicine practice, handing out glossy brochures about “Here to Help,” a system to help those suffering from mental illness and substance use. No drug was being promoted. It sounded “too good to be true.” It seemed fishy. I grabbed one of the brochures and checked out the site. Again, no drug was mentioned. The site was well done. Again: “Too good to be true.”
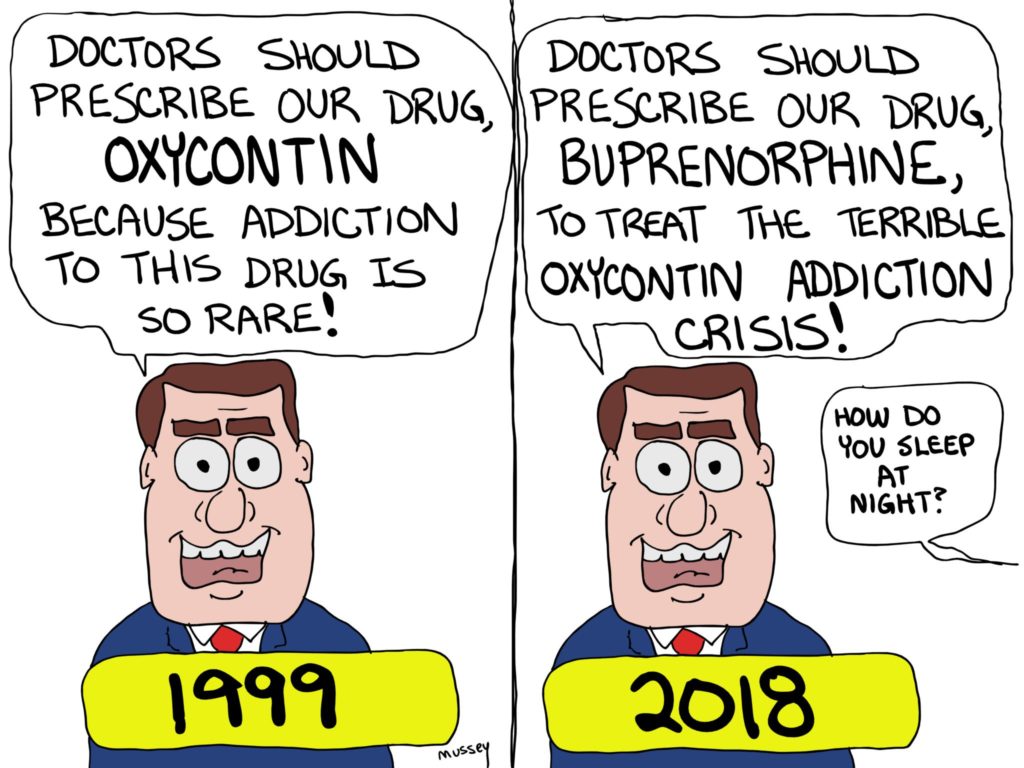
I Googled further and came up with links to Suboxone (Buprenorphine)and with a bit of investigating, it became clear “Here to Help” should actually be renamed “Here to Send You to a Doctor Who Will Give You Suboxone.” If the goals were worthy, why the subterfuge? At the same time, a publication for the American College of Physicians (ACP) was promoting Buprenorphine heavily. In fact, the supposedly unbiased publication printed a series of articles which read like promotional ads for Buprenorphine.
I actually sent them an email to complain. It is one of several promoting the therapy for primary care offices. If you can easily order Metformin, you should feel just as easy ordering Buprenorphine! Why not?
This year, the company behind Suboxone and “Here to Help” was indicted.
Key points:
- A federal grand jury sitting in Abingdon, Virginia, has indicted Indivior Inc. (formerly known as Reckitt Benckiser Pharmaceuticals Inc.) and Indivior PLC (Indivior) for engaging in an illicit nationwide scheme to increase prescriptions of Suboxone Film, an opioid drug used in the treatment of opioid addiction, the Department of Justice announced.
- According to the indictment, Indivior obtained billions of dollars in revenue from Suboxone Film prescriptions by deceiving health care providers and health care benefit programs into believing that Suboxone Film was safer, less divertible, and less abusable than other opioid-addiction treatment drugs. Indivior also is alleged to have sought to boost profits by using a “Here to Help” program to connect opioid-addicted patients to doctors the company knew were prescribing opioids at high rates and in a clinically unwarranted manner.
This week, the maker of Suboxone is settling by paying 1.4 billion dollars.
There are perpetual forces trying to manipulate doctors. Often the argument includes: “You have a moral obligation to …(insert dubious therapy).”
The rush to push all pain patients onto Buprenorphine may ultimately prove to become the standard of care. But, what I see looks very wrong. The amount of money involved makes me very suspicious. The sudden momentum is disturbing. I am seeing pain patients, not previously on narcotics, who are suddenly being started on Buprenorphine by pain clinics. This seems really bad. Such patients often come in complaining of fatigue, memory loss and depression. Then I see a drug list which includes Buprenorphine. Meanwhile, professional organizations, claiming to support doctors and our patients, too often just seem to go with the latest wave.









I recall the overwhelming pressure by the California state medical board to treat pain the way they saw fit; which, in my opinion, was excessive. Since I was the one writing the prescription and it was my medical and DEA license, I decided it was my job to determine what was safest for any patients I treated. The only two complaints I ever received from the medical board was by two patients who accused me of not treating them because I didn’t give them the narcotics they requested. Both complaints were dismissed after records were reviewed. I had practiced safely. But that is not what saved my a**. It was that I had written an extensive medical decision making process on why each patient was managed in the way I determined was safest and best for them. That is my job as the physician.
Fast forward all these years, I still have not changed my practice. Only today, it falls within the guidelines. I think the medical board was heavy handed and stepping outside of their zone in dictating how physicians fully trained in medicine should practice. Their job is to make sure the public is not harmed, not engage in crowdthink and use that as false policy to bully physicians into practicing bad medicine. They have never been held accountable for their actions. They were surely complicit in the opiate crisis as well.
I fear Suboxone is headed in that same direction. Popular practice rather than appropriate practice. Do what is best for the patient and you will never be wrong. My lifelong motto.
Re the comments above I continue to be surprised by how the role of JCAHO and state medical boards in the opioid crisis has been ignored. I am all for going after the drug companies as they did have a hand in all this, but people forget how regulatory agencies were gleefully along for the ride.
I am skeptical about Suboxone. I was certified to prescribe it some time ago and currently have no patients on it. The government sends mixed messages in that publicly they espouse buprenorphine, but then have a policy where DEA agents drop in unannounced to audit the buprenorphine patients and put your schedule an hour behind. Their approach sends the message that buprenorphine is a bigger threat than the narcotics that fed the opioid crisis in the first place.
As I said I currently have no patients on Suboxone. I have read statements by physicians that it works great and they have many successes with it, but in the FP setting I’ve had no long term success. It does have diversion potential and eventually every patient I’ve had on it has broken the written agreement i require. I think if it is part of a program with lots of counseling and support staff it can work, but that’s not possible in most small offices.
What is medically necessary. What is the best practice as detailed in your education,training and experience. What does current literature based on good quality studies say to do.WHAT would YOU do if this patient was your SPOUSE, CHILD, Mother OR FATHER.What would you expect for YOU.Would you use a narcotic or just tylenol, Motrin or Naprosyn. For depression mild to moderate would you use a SSRI, MAO OR TRICYCLIC ANTIDEPRESSANT. or just talk,counsel, tell them to exercise outside for 30 minutes a day ,every day, and in 3 months they are often ALL BETTER. Much more impressive to write a prescription?. Overused and Over rated. Magic Pill. No such thing. I base what I did on good studies, what my supervising physician recommended and Screw the Drug Reps AND Government, and Insurance Companies. They don’t treat the patient and Take No Responsibility. That falls on use as does Liability. To do otherwise endangers you and your financial future. That Ain’ worth it.As long asyou do what is Right based on good science, community standards of care, and latest studies with solid grounds you will be Alright. course all the people who wanted a pill will complain and say bad things about you. Sucks to be them.
Never forget, all this started over 20 years ago when government and quasi-government agencies decide they know better then physicians as to when opioids should be prescribed. All the pharmaceutical companies did was to go along for the ride.
Correct.
Until the JC is completely destroyed by a flood of lawsuits, justice will not have been served.
I have been detailed hundreds of time by Pharma reps and at no time was there ever a quid pro quo or did they ever have the power to alter my prescribing habits. Only the government had the power to that.
Amen.