Thank You Sir, May I Have More (Bulls**t)?

When I was a child in the ‘70’s, there was a very popular series on the air called, “Emergency!”. It revolved around Gage and DeSoto, two paramedics associated with the fictional Fire Station 51 and Rampart General Hospital ER. In the ER was Dr. Brackett the ER physician, Dixie McCall, the head nurse, and Dr. Early, a neurosurgeon(I didn’t know enough then to question why an NS was in the ER regularly…). It was that show that began my interest in the field of emergency medicine. Initially, I wanted to be a paramedic; however, I was impressed with Dixie McCall and decided I would be an ER nurse and eventually entered college as a pre-nursing major. Over the years and after obtaining more experience, I subsequently decided I craved the expertise and knowledge of a physician. I earnestly desired the ultimate responsibility of determining the care and/or management of patients. I had a strong sense that I would be good at making decisions in a crisis. I was right.
The moment I set foot in an emergency department, I knew I belonged there. That environment was a perfect fit–I am at my best when I have to react swiftly and with clarity. The challenge of being prepared to handle whatever entered those ER doors was titillating. 25 years later that excitement has not dissipated one iota. I thought I would never leave….until I did. It became an environment in which I no longer desired to practice and decided to take a respite.
When I trained, I learned about the history of how acute care medicine came to be. I’m extremely proud of that history because the founders of this specialty recognized that the public needed emergentologists. The changes they instituted, which included pre-hospital care, changed the course of medicine forever. Exceptional standards for emergency medicine were established and the quality of care improved. As a result, many lives have been significantly impacted–in a positive way. Being part of this family was an honor…then corporate medicine entered the picture.
I barely recognize my specialty at times. The priority of treating the sickest patients first has transitioned to “moving the meat”, a practice that inherently does not favor the sickest, but the least ill. This inevitably delays care to those who most need it. Waiting room times, length of stays, time to admission and other metrics meant to improve reimbursement has infiltrated, much like cockroaches, what was a wonderful clinical mecca of acute medicine. Patient education is compromised and patients are treated as commodities. Patient satisfaction scores have become the litmus test of one’s clinical performance. Yep, a popularity contest trumps the actual practice of medicine. And the art of acute care medicine is now being taken out of the hands of the medical experts and handed over to non-physician practitioners(NPPs) by corporate whoremongers. ER physicians are being forced to supervise and teach their replacements or become unemployed. The ones to whom we were expected to hand the torch, medical students and residents, are being pushed aside and their education compromised…all in the interest of supposedly saving money. I submit there is also one other less discussed reason. Physicians are notorious for refusing to take orders from corporate management, especially if it places patients at risk. You know–the conscientious docs labeled as “disruptive”. We tend to be passive creatures, but not when it comes to this–we are fervent patient advocates. We take the heat for being so…if we have to. Unfortunately for the C-suite, besides our oath, we are supported by the bylaws of every hospital which places the ultimate management decisions in the hands of the treating PHYSICIAN. They can’t have that, so they use practitioners who are not only cheaper, but less likely to resist the pressure placed on them because they simply do not possess the same authority to oppose corporate leadership.
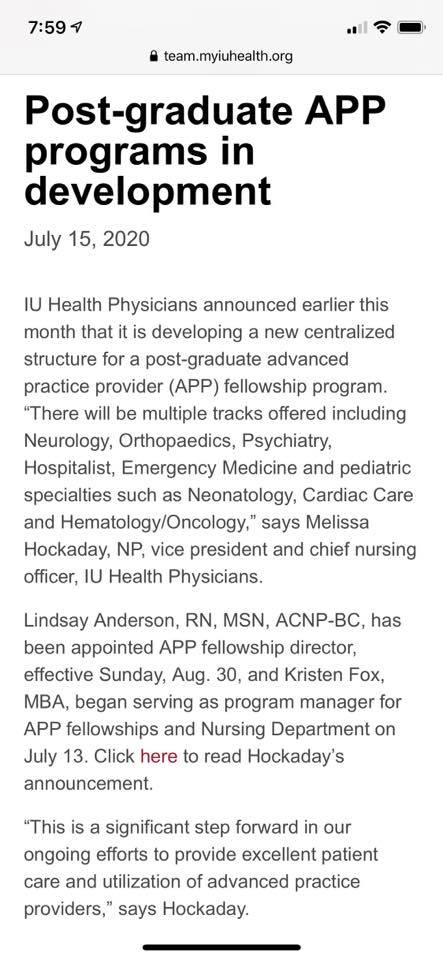
Nevertheless, the transition is happening. Physicians are fearful of losing their jobs, not understanding that the stage is being set for them to lose their jobs anyway. So they assist in the transition. The barely concealed actions by so-called academic institutions to replace physicians and/or minimize the significance of our roles on the healthcare team is reprehensible. The information page at the top of my commentary was recently posted by Indiana University Health(and abruptly removed from their website). While thousands of unmatched medical school graduates(and potential ER docs) sit on the shelf collecting dust because there are not enough residencies for them, IUH has begun an ER program for non-physician practitioners who have no requirement to complete the steps I did to become an expert in emergency medicine. There is no presumption on my part that the leaders in the Department of Emergency Medicine at IU initiated this process because I’m not convinced they did. I do believe they are being forced to sanction and assist in its formation based on the notice from IUH(see below) regarding other “fellowships” for the NPPs. There is no way in hell you can convince me that the ER residents(or most core attendings) in this program are in support of permitting non-physicians to participate in their ACGME mandated residency. If they are, I would be mortified. I question whether ACGME is even aware that IU is enabling this very questionable activity. In my opinion, the idea to develop “fellowships”(professional appropriation at its best) is a corporate one.
I am incensed and offended. I’ve been lecturing middle school, high school and college students on the value of education for over 30 years. Because education matters. Like other physicians, I worked my a** off to achieve what I have so I could bring the best that I have to my patients because if not for these selfless patients, I would not be the physician that I am. I also would not be the physician that I am had I not completed the standardized preparation and training that is mandatory to become a physician and that has worked, under the Johns Hopkins model, for 100+ years in America. Yet, an “academic center” such as IU has the audacity to not only promote, but brag that they are training NPPs to become “specialists” in Emergency Medicine, “specialists” who can then go on to “independent” practice states, work in an ER and tell patients they “specialize” in emergency medicine because they completed a “fellowship”. The potential to deceive the public is enormous. Eventually, because of programs like IU’s, my EM residency certificate won’t mean s**t anymore. My board certification, which required me to take TWO all day exams, one written and one oral, a year apart…won’t mean s**t anymore. Because IU has found yet another truncated pathway(besides legislators) to enable NPPs to become emergency medicine “specialists” rather than effectuate the seven years that was necessary for me to achieve the same. This does not only apply to EM, but also the other specialties in this link to IU’s “APP fellowships”(https://iuhealth.org/professional-education/advanced-practice-providers/advanced-practice-provider-fellowship). Imagine that…a fellowship without completing medical school or a residency. So much for valuing physicians and medical education. Shame on IU. I sincerely hope that as academic programs continue to develop these ER “residencies” and “fellowships” for NPPs(IU is not alone), all the while ignoring unmatched medical graduates, emergency medicine’s umbrella organizations and societies, including the American College of Emergency Physicians(ACEP) and American Academy of Emergency Medicine(AAEM), take note and address this corruption of our specialty accordingly.
Medical students applying for residency, take heed.??
Get our awesome newsletter by signing up here. We don’t give your email out and we won’t spam you.









My alma mater (MD and FM residency) is now operating a Nurse Practioner “Residency” program, with such rigorous curricula as supervised (by a NP) outpatient clinic….where each “Resident” has to see one patient per half day of clinic. And for that, they will receive full resident pay and benefits.
Who exactly is responsible for replacing ER physicians with NPs?
Is it the hospitals/hospital corporations?
Or is it the mega-groups (often owned by private equity) that contract with the hospitals to provide coverage?
Any or all of the above, Stewart. Most likely someone with no medical experience.
I suspect the answer is yes
I am a retired Operating Room Registered Nurse, my daughter is a Emergency Physician that was recently, along with several other seasoned Emergency Physicians, replaced with mid levels. Seems to me if the general public was made aware of this horrendous happening all over our great country they would be outraged as I am. If there are persons that has the ear of the honest media please put this information out there so the people will be aware.
This is unfortunately common. We are informing the public and legislators. A patient/physician advocacy group to which I belong, Physicians for Patient Protection, supports and has a job board for docs displaced by non-physician practitioners(NPPs). Please have your daughter contact us. We are politically active and oppose the replacement of physicians by NPPs as well as bills that promote their unsupervised practice.
Great post.
“I sincerely hope that . . . emergency medicine’s umbrella organizations and societies, including the American College of Emergency Physicians(ACEP) and American Academy of Emergency Medicine(AAEM), take note and address this corruption”
That made me laugh at loud. Surely, no one has been complicit in creating this disaster than the parasitical organizations that claim to represent us.
This will make healthcare worse and more expensive.
An the malpractice plaintiffs attorneys extremely happy and well paid. And after millions have been paid out, the powers that be will find out that physicians weren’t so bad after all.
You’re giving your age away Dr. Newman… I remember “Emergency” too, but I go further back to Dr Kildare and Ben Casey. I am pessimistic, between what the government has done, and Covid-19, physician medicine is dying. I am glad I am in my last years and I feel badly for those coming behind.
I cannot understand why anyone would want to put their life on hold while incurring tremendous debt for a medical education today, just to take a job as an employee of a health care system.
There are penalties for our capitalism……we must now be judged by how profitable we are. Dollars and cents are easily quantifiable. So are patient ratings.
We do not make any more money by taking care of complicated patients.
It is ironic. In the old days we always used to joke that someone could obtain a doctorate degree from the back of a comic book. Now most patients consider anyone with a white jacket a doctor.
I trust this training program includes fashion guidance- go for the labcoat, not the short white jacket (that was for the medical students in my day).
In my specialty we were/are always worried about optometrists enlarging their scope of practice through state legislation- and they have! Now there are discussions about inviting optometrists to our annual Academy meeting- that ceased right after the Covid outbreak because the meeting was cancelled. But we are continuously bombarded to contribute to every state that has a pending Optometric Scope of Practice bill….which happens all the time.
An organization to which I belong, Physicians for Patient Protection(PPP), opposes all bills designed to expand optometrists scope of practice(SOP) if they segué into surgical procedures or any other practices that should be performed by residency trained opthalmologists. None of these legislators who pass these bills ever take into account who will manage the complications from optometrists performing outside their SOP. The assumption is that those patients will be sent to the opthalmologist to repair and manage the f**k ups. Part of being an expert in a field is that one must possess the ability to manage one’s own complications. Nope, they want to do the fun part that allows them to be paid handsomely for their work and that is where their responsibility ends. I wrote about it in another blog for Authentic Medicine(https://authenticmedicine.com/2020/05/what-kind-of-fkery-is-this/). PPP generally remains abreast of these bills because our organization is a multi-specialty organization. As such, our opthalmology colleagues keep us informed and then we create calls to action to oppose the bills by bombarding legislators with letters and phone calls. It works.
I got out and retired at 63.5 years of age and suggest that anybody in this day and age save like heck and bailout when they can. Don’t have too many kids. That helps.
Nice positive news on a Monday morning. Medicine has been commoditized and corporatized. How much do you need to pay a person to generate a billable CPT? That is what the CFO and insurance company accountants want to know.
I went into ophthalmology because it was a niche specialty back in the early 1980’s- I did not mind being the sole ophthalmologist in 2 rural towns and accepting all their ER calls- from the ER docs, and back when payments were fair and the workers comp not burdensome. Things changed. I was grandfathered out of ER call. NP’s and PA’s would dump on me, saying they did not know much about eyes. I am a doctor- I will have a curbside consult with another doctor, not a PA! Insurances started tightening up- reimbursals fell. Workers comp required tons of paperwork. Now I refer patients
to the ER who call with eye emergencies- floaters, injuries, etc., if they are unable to pay copay and deductible or if there insurance sucks. So it is the other way around. The hospital cannot refuse to accept them. EVERYTHING HAS CHANGED- and I do not go to the ER any more and my malpractice company told me never to accept a phone call from the ER- because that initiates my liability. So everyone is on their own now.
Great post, Doctor. Thank you for so eloquently composing how many of us feel. I appreciate your posts.
Fred, I will join you in complimenting Natalie on her eloquent narrative.
I concur.
Strong work, Dr. Newman.