Should MDs/DOs and PAs Truly Team Up Outside the Office?
Recently, this blog criticized the doctorate programs of PAs. The obvious reason is the ultimate confusion it may cause. What I have learned from some PAs that I know, as well as comments by other PAs, is that these doctorate programs are more to keep up with NPs. The NPs are seemingly favored by adminisrators because of their cheap cost and their politically enabled ability to be independent. It seems to me that PAs are in competition more with NPs and don’t want compete with doctors. Am I wrong?
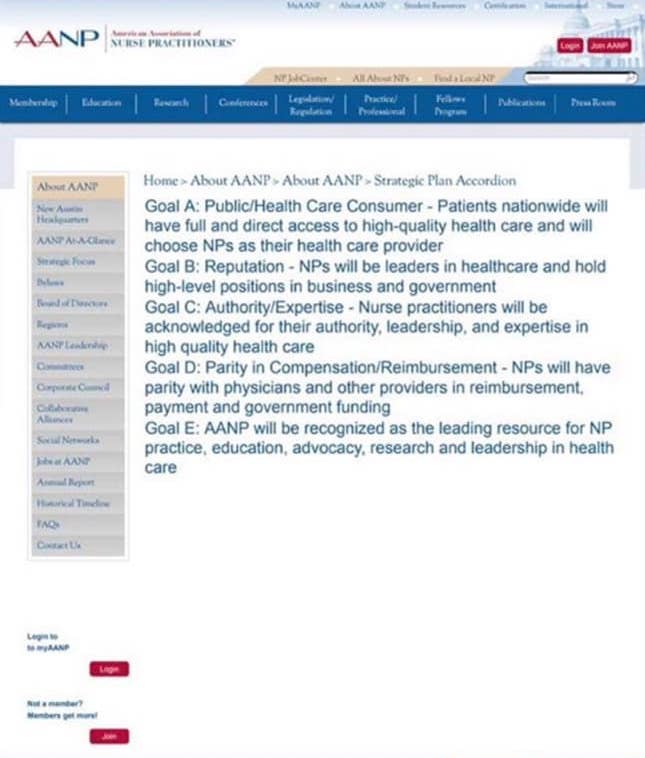
What you can see above are the goals by the AANP. They have now gone on record stating that they want patients to “choose NPs as their health care provider”. It is obvious that they no longer what to be collaborative with doctors, but instead choose to be competitive. (I cannot find these goals anymore online. They have been deleted or are hidden).
For doctors:
- Should you continue to oversee them?
- Should you continue to use them as a source of income?
- Should you refer a patient to a specialist and allow that patient to see an NP as the consultant?
For PAs:
- Do you see a role in collaborating with doctors?
- Do you hold firm not to try and be independent and use you doctorate to confuse patients?
- Work with doctors to fight against the NP political machine, which claims to have equality in training and care?
I think there is an opportunity for MDs/DOs and PAs to work together outside the office to stop the madness portrayed by the image above. What are your thoughts? I would love to hear from all sides here.
(Any vicious attacks and comments by NPs will be deleted).









https://www.thedailybeast.com/rock-doc-jeff-young-the-wild-story-of-a-reality-tv-wannabe-accused-in-pills-for-sex-scheme
Yeah. I get all that. You cannot deny that Obamacare injected a huge dose of steroids into these situations. And now there are major problems. EHR comes to mind.
And WW2 started with the reorganization of Europe after WW1. But it didn’t break out into flames until 1939.
So yes I am blaming Obamacare.
Could you imagine if the AMA and other physician organizations had balls like the AANP? They’d have this healthcare mess cleared up in no time!
Parity and commercial competitiveness with NP’s is exactly what it’s all about- economic survival is the game. PA’s by my experience are team players and want and intend to stay operational with collaborative physician partners. It is NOT about superseding that role, nor about independence of practice. Candidly, for practically all patient care/ service professions, the doctoral degree is the entry/practice level degree,i.e, clinical psychologists, PharmD’s, PT’s, optometrists, chiropractors, etc, etc, etc.
No one balks at their being at the doctoral level- so why can’t PA’s have doctorates as well?
I’m a practicing fam prac and prim care PA, entering my 42nd year of practice- the first half of that in the US military, where I frequently supervised physicians, PA’s and nurses. None of us for a minute presumed that professional positions were in any way different. PA’s, myself included, remained the partners of our collaborating physicians; over my career, about equal parts MD’s and DO’s.
Degrees do not change professional relationships or statuses.
In my opinion it’s stunningly short of professionalism and character to presume otherwise.
Stephen J Chirigotis, PA-C, MPAS
(Major USAF, Ret)
I’m a NP and it drives me crazy when we send a patient to a specialist and they are seen by a mid-level (I think it’s a little insulting). I became a NP so that I could help in the office at a different level (when doctor’s cows are out, he can leave to take care of them and the scheduled patients are still seen). I’ve worked with my doctor in our rural family practice office for over 30 years. He’s a smart guy. If he needs a specialist to see a patient it needs to be another doctor, not an extension of that doctor. The training/education is not the same!
Just my 2 cents worth as a former PT. The conflation of various health professionals to “doctor” has always baffled me. Why would I want to take on the responsibility of direct access and thus pay the price if the patient’s back pain was due to a metastasis or a kidney infection rather than sprain/strain? I’ve worked with PTs with conflated degrees and never felt they were that much more skilled than myself and they certainly didn’t have the pharmacology skills or radiology skills that an MD needs.
As a current medical transcriptionist, the notes I’ve transcribed at the family practice level from midlevels tend to be more easily understood but other than that have not given me confidence to choose them as my PCP. OTOH, the notes dictated by midlevels for specialists truly impress me. The specialists do not seem to use them interchangeably with the doctors but rather as a true assistant, taking care of things like cast removal, stitch removal, wound checks, triage, basic H&P/ROS so the specialist has extra time for what the patient was referred for. They’re also important in patient education and seem to work more closely with the physician in charge of the patient’s specialty care.
I think adding midlevels as PCPs has contributed to my primary frustration with US medical care as I age. It seems the PCP does very little any more but prescribe routine meds and refer out. My husband requires assistance with memory and driving so I have to attend him during all visits. It seems all we do is try to keep track of appointments with urologists, radiologists, pain management, orthopedics, etc. When I took my dad to a geriatric specialist it was pretty much the same – referrals to neurologist, psychiatrist, urologist, etc. etc. I understand knowledge in these areas has grown greatly but it’s still frustrating to try to get the PCP to take over the mundane aspects of treatment once the specialist has diagnosed the problem.
“Alexa, what does society get when they choose ‘cheap’ over ‘quality’?”
Doug, see what Obamacare hath wrought.
Only the government taking over health care would allow, as you call it, this madness.
Obamacare is a truly a Pandora’s Box that has been opened and the evil has flowed out like poisonous fumes.
If we had Republicans with spines, it would have been removed, stem and root. But then we were gifted with McCain.
It is SO evil and yet they show interest no longer. To me, it screams for removal.
The blog post by the NPs you referenced is nothing more than another level of evil. We are standing above a bottomless pit.
“Obamacare is a truly a Pandora’s Box that has been opened…”
Except that, as you are no doubt aware, the structure of “Obamacare” was a Republican invention, created as a riposte to Clinton’s attempt to introduce universal coverage in the 1990s, and then resurrected, zombie-like, by the Democrats, who, it seems, thought that since it was their own invention, the Republicans could not refuse it.
It was never a good idea, because it was invented by people who were opposed to the concept in the first place (which is not to say that I think I have any better ideas).
So, that Pandora’s box that was opened… was opened by the Republicans.
The move to replace MDs with NPs and PAs was well underway prior to Obamacare, being pushed by hospital corporations and insurers (i.e., good old capitalism).
When we blame Obamacare for all the problems in the medical care system, we just look ill-informed.
Nurse practitioners first started in 1965, long before the Affordable Care Act came into being. Stop trying to blame it and blame the politicians on both sides who are trying to get away with cost reductions at the expense of people’s health.
1965, the year these economics were permanently corrupted by the passage of Medicare, that aimed us toward all these egalitarian triumphs.
Yeah. I get all that. You cannot deny that Obamacare injected a huge dose of steroids into these situations. And now there are major problems. EHR comes to mind.
And WW2 started with the reorganization of Europe after WW1. But it didn’t break out into flames until 1939.
So yes I am blaming Obamacare.