Education and Training Matters
The above comes from a DO publication. Here is what they said:
In recent years, many different types of non-physician clinicians have sought to practice medicine independently of physicians, despite the fact that doctor training requirements are significantly more rigorous and comprehensive.
So far this year, the AOA helped defeat scope-of-practice expansion efforts in Indiana, Hawaii and New Hampshire. The AOA opposes any legislation or regulations that would authorize the independent practice of medicine by an individual who has not completed the state’s requirements for physician licensure.
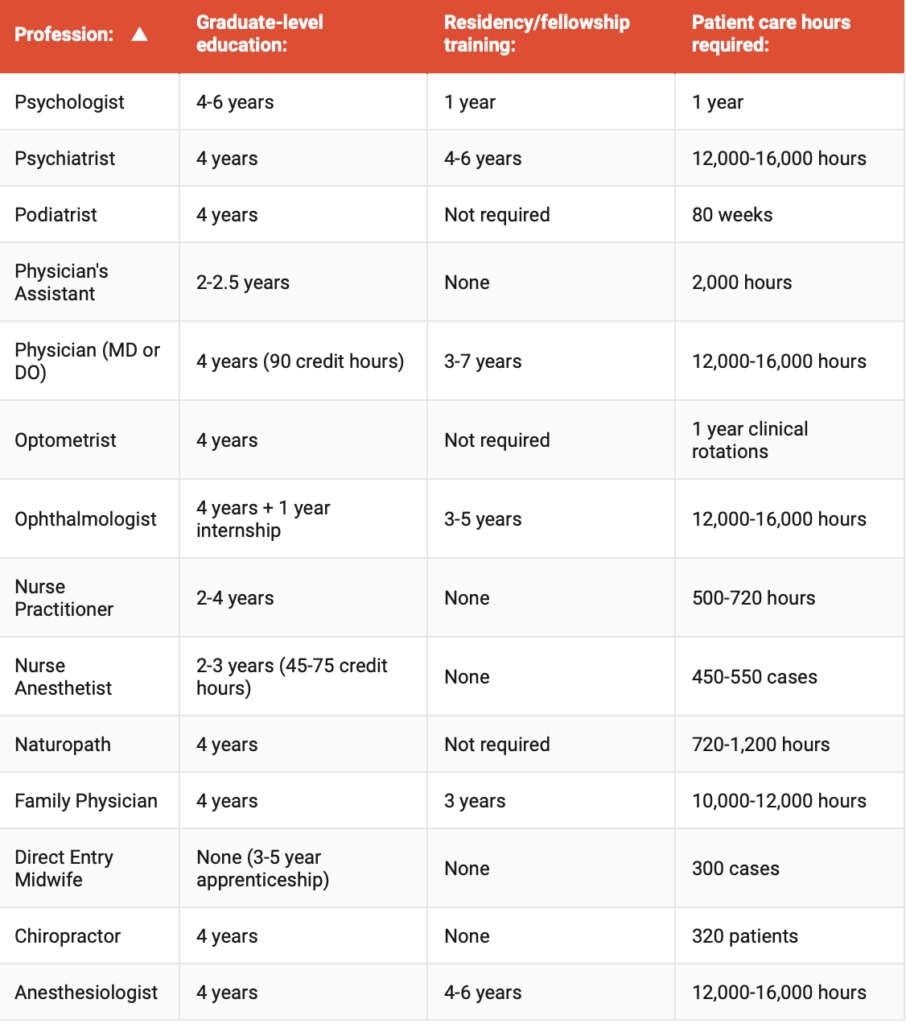
Non-physician clinicians are highly skilled professionals who are essential to the the health care system. Their education and training are not equal to that required for fully licensed physicians, and the AOA supports their work in physician-led health care teams. The chart below shows the stark contrast between doctor training requirements and those of other health care professionals.
Thoughts?









The numbers speak for themselves.
The article is concise and simply compares the hours and or years of didactic and clinical training. A seasoned clinician MD or DO who is board certified and internship and residency/ fellowship trained is the gold standard. All else is substandard. Even within the ranks of DO and MD physicians, non board certified physician’s are considered substandard. Even though these physicians attended medical school, internship and residency training. Comparison of any other medical professionals to the gold standard is simply moronic.
Experienced NP here. It is so unfortunate this topic has gotten ugly between colleagues. The issue is very multi-faceted. Let’s start with the fact that I DO NOT practice medicine. I practice advanced nursing. I treat the usual, the typical; usually with as much education and counselling as pharmaceuticals. I don’t claim to be able to tell you what variety of Zebra (or is it a Gnu?) I’m dealing with, just that it’s not looking/acting like most horses and that’s why I’m referring on to you, dear doctor (possibly with my suspicion that it might be an Ox). And yes, my post-Master’s NP program had less than 1000 hours supervised clinical practice. But I had over 25 years ICU experience when I was the eyes and ears of the physicians I worked with, determining if a patient situation fit the treatment guidelines (AKA standing orders) in place or not; does my education and experience allow me to appropriately deal with this or do I need to involve someone else? Maybe that someone else was resp or speech therapy, maybe one of several medical specialists. I can only speak for the legal situation in Indiana. We are required to do a weekly 5% after-the-fact review of prescriptions, with our “collaborating physician”. Professionally, we are NOT asking for an end to collaboration, but an end to this paperwork exercise that does nothing to promote patient safety. And we are NOT asking to hold ourselves out as specialists in anything but advanced nursing – to practice to the extent of our own (as individuals) training and expertise w/o useless paperwork exercises. NP’s have been around for over 50 years – but only a phenomenon in the last 20 or so. Our educational requirements (especially required practice experience prior to embarking on an advanced role) will sort themselves out and standardize, much as physician training did after the Flexner report 100 years ago. In the meantime, the title’s right – education and training matters. NP’s are asking to be allowed to use their education and training without administrative and bureaucratic restrictions that in no way effect the quality of care provided.
See all articles written on this site by Robert Duprey MD
Chamberlain University
Earn an Accredited DNP Online
Tuition & Fees: $21,655
Pay Only $375 per Month
14 Courses
24 Months
100% Online Coursework and Local Immersion
So, would anyone in medicine let this graduate take care of your family unsupervised? I’d bet over 90% wouldn’t. Why would anyone expect the uninformed public to do the same?
But the MBA trumps them all. The big push to fan the flames of the internecine rivalries within the Healthcare professions is to restructure the PROBLEM OF LIABILITY that is still attached to the professional practitioner. In order to get American McMedicine to cost less and become more profitable to the LLC’s that own it, one needs to “hand autonomy back to the customer” by reducing the “practitioner” to the level of the clerk at the perfume counter. Let’s get rid of the “ask your doctor” phrase in advertising McPharmaceuticals to the highly self-impressed customer/patient. Let them pick out a diabetes regimen. It works for chiropractors!
Once the vendor’s responsibility is diluted to the level of chainsaw salesman at the big box hardware stores, let’s see what happens. I hear that fermented carob seeds are the equivalent of insulin, you hear that too?
Jesse Belville,PA-C for 43 years. I am a PA, my role is to handle the routine health care problems and do 70 to 90% of what my Supervising MD or DO does. My role is to increase access to care, improve the quality and efficiency of the practice,while freeing my Supervising Physician to see and care for his more complicated patients. Making his life more productive, lees stress, better satisfaction of his patients in his care. Time to see and care for him or her self and family. That was the Ideal… Instead, I practiced at the far limits of my knowledge, 60 to 100 hours a week, often used and abused, poor supervision, and when I referrred to my supervisor physician, he would not come back me up,which I documented. Soon I found another position. I love being a PA-C. If I could not be a PA, I would be an RN or EMT/Paremedic. I love helping one person at a time. I dislike the politics and NP’s and some PA groups trying to become /have the authority of Physicians, without the skills or training. Thank You. Now get the rest of the Physician Groups off their butts and take Control of the Medical Profession Again. Please. Stop this power grrab by the Nursing groups and other interested persons. Now
Well put. If someone wants the authority and responsibility they can take on the education that ms required and stop lobbying for a short cut to a higher income. Go do something original that helps the system we’re in and stop trying to reinvent the wheel. As a PA, the role is not to be competing with physicians, it’s to be assisting them and vice versa. When we need help, they need to be present, and we need to be actively working to help take care of some of the more nuance medicine that does exactly necessitate a physicians presence.
That said, I also would be in support of more PA/NP-to-MD programs which needs to take into account the amount someone has practiced.
There are physicians doing just that–I belong to such an organization. We fight the unsupervised practice of NPs at a legislative level. It is preposterous. There is no question that physicians are partly responsible for this mess of nudging those not trained in medicine to believe they can actually practice medicine. Happened when we relinquished our leadership role. Much of it had to do with metrics. The time I had to closely supervise PAs(I’m EM, when I trained, there were no NPs in the ED) was generous. The demand to meet metrics, with the increase in the number of PAs(and subsequently NPs) I was expected to supervise, forced me to either comply or risk losing my job. I chose to continue to supervise and yep, I was taken off a few schedules. Many docs can’t or won’t do what I did, hard to be unemployed. I appreciate PAs such as yourself who desire the supervision, guidance and collaboration. It worked well when we worked as a team. Now we function in silos. Where there is no leader, there is only chaos and substandard, mediocre care.
It is my personal belief that most PAs do not wish to have independent practice, they are pursuing that avenue as a means to employment survival in light of the NP push for unsupervised practice. The irony is that PAs are trained in the medical model and speak the same language as physicians. Your practice is designed to be compatible with ours. Nursing is a different model and discipline altogether. Their autonomy fell under a nursing umbrella and they generally worked in conjunction with a primary physician. Hence, the vast number of family nurse practitioners. The relationship was symbiotic. Somewhere along the way that autonomy segued into medicine and they began practicing in areas they do not belong. With no understanding of medical pathophysiology or pharmacological management. Years of nursing does not equate to the practice of medicine—it never has. The number of patients sent to me in the ED from NPs who simply had no idea of how to manage a patient was astonishing. Patients that would have been easily managed by a primary care physician. The quality NPs with whom I worked years ago held themselves to a standard. Nursing was held to a standard. That is no longer. Anyone can become a NP. Hell, anyone can become an RN. No competition whatsoever. And where no competition or standardization exists, how can there be consistent quality? There can’t be. I no longer supervise or precept NPs. Not worth my license.
Is Farrago really a physician? This article seems like it was written by a complete imposter! Most of this information is completely inaccurate, and where are your sources?! It wasn’t that long ago that MDs completely ostracized DO’s physicians. Please don’t downgrade the internet by posting bullshit like this whoever you are!
The article was from the source linked. If you have a problem with it then ask them.
It’s fairly accurate. Your parroted objection from the NP talking points is completely invalid. MDs ostracized DOs merely for the different initials and politically separate schooling system. DOs were the first to adopt and implement the Flexner reforms that revolutionized medicine. The same reforms that the concept of NPs is designed to subvert. DOs have always had the same level of education and training as MDs. NPs aren’t even close to 1% of that education and training.
Psychologists have no medical training. This chart is misleading. Separating psychiatrists from other physicians perpetuates the stigma that we are not “real doctors”. They need to clean that up. The chart only serves to give psychologists ammunition to fight for prescribing privileges.
The article was from the source linked. If you have a problem with it then ask them.
The chart doesn’t claim they do. But conversely, psychiatrists don’t have any psychological training. Develop some reading comprehension skills.
They have separated out opthalmologists and anesthesiologists as well. I think it is those specialties that have non-physicians trying to compete and obtain privileges to which they are not entitled. I don’t believe it is meant to indicate they are not physicians.
Hi, Physician Assistant here.
A couple things Dr. F. So often I see PAs and NPs grouped together and its a little confusing to me and I’ll get to that. The differences in education you listed above are absolutely correct. But it goes further: PAs are trained following the medical model. It’s based off the advanced/shortened medical school training that were started during WWII actually. NPs follow the advanced nursing model.
This next statement might cause a kerfuffle. From that we might conclude that medical school and residencies are too long. That perhaps there are ways to still practice quality medicine without substantial debt and 7 years minimum of dedicated life. Further, the limited number of residency spots, limited number of med schools guarantees that there isn’t a chance in hell that Docs will fill the demand. (unfortunately with all the online NP schools current estimates suggest the market will be saturated by 2025).
Second- PAs follow the medical model and our PA boards in general accept the fact that our training was designed so that we work with doctors. We are looking for some changes called optimal team practice. Part of this means having our own state boards. Currently nurse practitioners are regulated by the nursing board. Docs by the medical board and PAs by the medical board. Another large part of this is that the oversight/collaboration/supervision be decided at the practice level. This is important because a PA practicing for 10 years shouldn’t be required to have his/her hand held but a new grad or somebody changing fields realistically would. The important point I’m trying to make is, NPs want complete independence. They say that. They also want to be called doctor in the clinical setting which I think we all agree can be inappropriate if not differentiated from MD/DO.
PAs cherish our relationships with the doctors we work with. But with OTP, I won’t be treated the same as a new grad. Healthcare should be a team approach. We all have our roles.
Might be worthwhile to spend some time educating yourself about the differences. I think if you read more about OTP you’d see it as a reasonable and fair approach to the changing frontier of medicine.
https://www.aapa.org/advocacy-central/optimal-team-practice/
We really really would love to stop being grouped all together.
Just curious why psychiatry is a separate category from physicians. Psychiatrists are physicians. They are MD or DO.
Psychiatrists go to medical school, not podiatry school or optometry school. There is no psychiatry school. They are physicians, not providers.
I think he is comparing psychiatrists to psychologists, similar to the way he compared optometrists to ophthalmologists and CRNAs to anesthesiologists. Many non medical people don’t understand the difference.
“He”? I am just using the image and reference from the article. Feel free to take up any discrepancies with them.
I am using the reference from the article. You can surely take that up with them.
Too bad you picked Family Practice…I guess you weren’t pretty enough for Derm or cool enough for Ortho. bahahahaha
They are absolutely right. MD/DOs have significantly more training than any other health care practitioner. For NPs or CRNAs or anybody else to compare themselves is just obfuscation. It has long been said that you can’t diagnose what you don’t know, and they don’t know what they don’t know. They often call their observational periods “fellowships” or “residencies”, but it is a bastardization and mis-use of the words.