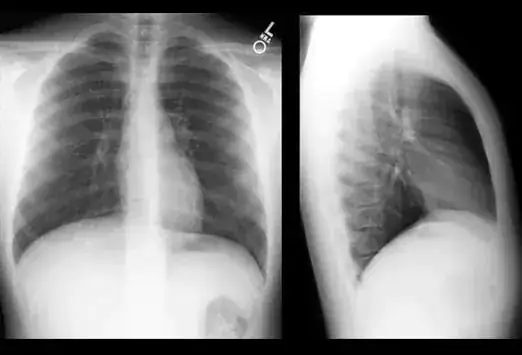
Whatever Happened to the ROUTINE Chest X-Ray PA and Lateral?
In the old days, when you admitted someone to the hospital for ANY reason, they got a Chest X-Ray PA and Lateral. If they were really sick, it was a portable film, which was felt to be suboptimal and warranted a good PA and Lateral film as soon as the patient’s stability permitted.
Flash forward to current practice:
Most patients are admitted without getting a Chest X-Ray. If, by some miracle, they get a Chest X-ray, it is a portable film of horrific quality. No one feels any obligation to get a good PA and Lateral film. If there is any sort of chest pain or breathing issues, the patient gets a Chest CT. More often than not, since most of us don’t have totally normal lungs, something gets seen. Maybe you see an apparent pneumonia on the chest CT which was not seen on the portable chest X-Ray and was never suspected in the first place. It doesn’t matter. Now, the case warrants IV antibiotics. Without any further imaging done in the hospital stay, the patient’s discharge instructions from the discharging physician extender advise lung x-rays in one week to follow-up.
“Lung x-rays?”
You didn’t see a pneumonia on the miserable portable Chest X-Ray you got in the ER (if the pneumonia ever really existed). Does that mean you need to get another Chest CT, instead? In a week? What about the old advice about waiting 4 to 6 weeks before imaging to check for resolution? Maybe you could have seen something in a decent PA and Lateral film prior to discharge which would have guided your future planning?
It doesn’t matter. The hospitalist physician extender is long gone, but is covered because follow-up advice was given.
So…. What happened to the good old “Chest X-ray PA and Lateral”?
If you have any sort of stroke or other serious complaint, you never get a Chest X-ray. Apparently, that is considered wasteful. That means the huge lung tumor which is causing all sorts of systemic trouble is totally missed.
Chest X-rays were basic “reflex medicine” in my day. If you dared appear at the feared “Morning Report” as a medical resident and did not have the chest X-Ray ready to display on the view box, you better be prepared to have your head chopped off by the supervising physicians.
Now, we pretend we can cherry pick who REALLY needs a Chest X-Ray.
How many times have you placed your stethoscope (you remember those, right?) on someone’s chest and heard all sorts of horrible stuff you never predicted would be audible. That’s why we do physical exams even if we don’t think it is necessary for the patient’s problem. That’s why the admission Chest X-Ray and EKG were essentially extensions of the admission physical.
Not anymore. We think we are smarter than that! We pick a couple of complaints and steer the patient into a computer pathway where we do the absolute minimal evaluation.
Meanwhile, we still get side tracked. You may be bleeding to death but the EMR demands you enter your flu shot status before it will let you move forward. “Do you feel safe at home? Do you exercise every day? I’m sorry, but I need to enter these answers into the EMR and I can’t understand you because you keep choking on your own blood…Wait! That reminds me of something I was going to do…but now I can’t remember!”
There was a logic to the old school of Internal Medicine. You looked at the films yourself. You also reviewed all X-rays with the radiologist every day. You did a gram stain on sputum and you looked at the blood slides when a CBC looked funny. We were always learning and the more we learned, the more we realized we still did not know enough. Chest X-Rays are cheap and they often show so much more than you imagined.
Bring back the routine Chest X-Ray and make it a good old fashioned PA and Lateral!!!









Nobody examines patients any more anyway, or at least, not well. I have to say during my dad’s last illness, watching the NP in the ER attempt to ascultate his lung over his left iliac crest did not fill me with confidence.
Yep, they show more than you imagined. Shadowing in the left lower lobe. Ct recommended. Ct shows nothing. But there is a cystic structure in the thyroid and several cysts liver. Image those. Nothing aggressive looking. Just recommend fna to be sure. Small bleed. Bigger bleed. Remove thyroid. irritate recurrent laryngeal nerve. Filler in vocal cord. Causes tendency for aspiration pneumonia. Recommend a chest X-ray. This is from the if you give a mouse a cookie and a moose a muffin series.
Yeah, right. Medicine has been replaced by “health care” – whatever that means on any given day – and anyone working in it is being continually squeezed by bean counters on one side, and the lawyers of vengeful patients on the other.
Experience and judgement don’t count a damn.