The BMI Dilemma
The BMI that we are all obligated to record on every patient every visit – I think it’s time we updated what and how we talk about these to patients.
I will give you my opinion here (it’s a blog, not a medical journal.) But what I believe is that these “normal” were set in the 1970s with a bunch of skinny drug-using hippies in California. We have changed – as a global people, but certainly as Americans. We are, in a word, fatter. I weighed less in the 1970s than I do now, so it is logical that it is true of everyone. I was 10 years old as the 70s exited, but still…
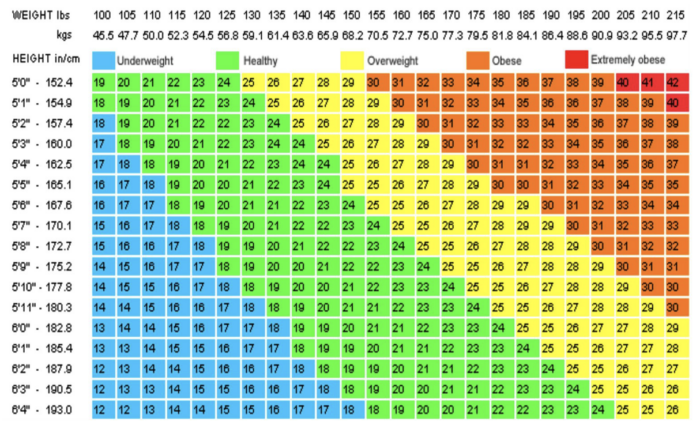
So, I propose we shift the BMI tables. Truth is – between BMI 25 and 30 there are not medical reasons to lose weight (it’s a stretch, but there might be orthopedic reasons.) In that range losing weight to below 25 will not reduce heart disease, will not prolong life, and if any blood pressure reduction it will be short-lived only. Plus, it is just nigh on literally impossible (says I, who sits usually at 27 and am now currently a 30.)
So I further propose calling “normal” BMI 19-30, overweight 30.1-35, Obese 35.1-40, morbidly obese above 40.1, and underweight below 19.
As it stands now the BMI chart is frustrating and shaming without current evidence. I was thinking about what external things do we have around us that cause body shaming, guilt, and despair? The following are a few things I thought of:
- Cosmo magazines for women -even the super hot models are not super hot enough to be included in the magazine and many have Photoshop help to be that attractive and sexy.
- The Speedo and/or thong for men. An anorexic John Holmes would still look like a pudgy toddler in those things.
- Skinny Jeans for any gender. Two words – Muffin Top.
Any other ideas of shaming things that we allow?









Please see above the link for “BMI Camp”. One of the most hilarious sarcastic articles from, I believe, the old Placebo Journal
No link but I remember writing it.
Would it not make more sense to determine lean body mass, percentage of body fat, rather than BMI?
I “fired” one doctor who, after my yearly exam, always had only one thing to say: lose some weight, i.e., you are too fat. At the time, my BMI was 27.5, and I was in my early 70’s and generally healthy but knew I needed a careful look at my thyroid functioning–which he ignored. I switched physicians and found one who actually cared about my overall health, who also discovered that I had developed antibodies to my thyroid (not using the exact terms here but you probably know what I mean). My BMI is currently at 24.5, achieved by the daily intake of my thyroid meds, AND months of exteme calorie counting and a great deal of exercise. To stay there means at best two meals a day, and a dessert-type food maybe once a week, or better, once a month.
Saturday night, I was at a Valentine’s Day dance at a local Country Club, i.e., think “wealthy people.” The rich tend to be a bit slimmer than the less wealthy, and yet perhaps 20% of the women there had “healthy” BMI’s and they skewed quite young. The whole thing is ridiculous.
Also in the diabetes column, you can add non-diabetic, prediabetic, diabetic, and uncontrolled diabetic.
Let us document how many cigarettes were smoked for how many years and how much alcohol of what variety is consumed on what basis.
My patient population is OLD. We are making it more and more difficult to simply enter data into the EHR
Many of my patients take 10-20 different drugs and supplements.
Do my EHR people who input this data have any leeway to cut corners? Do I get paid more for better documentation?
For Diabetics: I rate by The Good, The Bad, and The UGLY. (Blame the movie title, not me; e.g. https://en.wikipedia.org/wiki/Fat_Bastard ) The Diabetes Rating seems to help with treatment triage.