IOM Adding More Social Metrics
In another attempt to destroy the time allowed for patients to see doctors, the Institute of Medicine is now recommending all electronic health records be equipped to record and track 12 social and behavioral determinants of health.
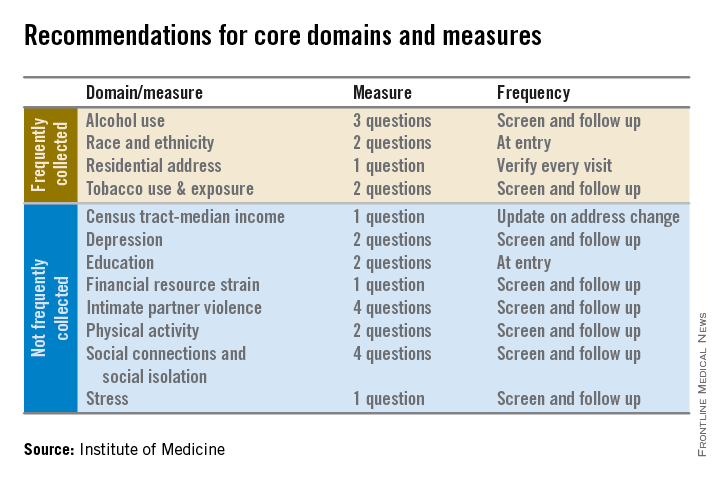
In addition to measures that are routinely collected now – race/ethnicity, tobacco use, alcohol use, and residential address – the committee advocated that electronic heath records (EHRs) should be able to capture:
• Educational attainment.
• Financial resource strain.
• Stress.
• Depression.
• Physical activity.
• Social isolation.
• Intimate partner violence (for women of reproductive age).
• Neighborhood median household income.
At what point do doctors say enough is enough. I know I did. Why is there no push back on this crap? Why are we such pussies?









Hey, hey….I ask alot of these questions, but for different reasons.
Alcohol use: d’you like stouts, IPAs, brown ale or Maker’s Mark?
Tobacco use: got any good cubans?
Residential address: just so I know the correct address to send you the AK-47 you just bought from me
some of they are valide and ones we ask on a routine basis, particularly intimate violence, but does there really need to be a metric on these?
This will (also) be used to indoctrinate med students and residents into the mindset that they should “care for the whole patient” – that patient now to include the neighborhood. It’s like the AAFP’s cultural competency module, telling me that I should automatically care about the customs and even language of the local immigrant clique – I don’t. Likewise I have every desire NOT to know about anyone’s financial resource strain, social isolation, or neighborhood median income. None of my business. In fact if practicing medicine has taught me anything about people, it is to narrowly focus my interest when questioning patients, and mind my own damn business.
I read a lot. I mean, A LOT. And this is some of the best stuff I’ve read in a long time. Sometimes the comments aren’t inane!
“What can we say about a mostly-Black, mixed-race girl who lives in government housing with her sister. Her mother has not been employed for most of her life. We know all about little Malia’s suffering. Her father has been engaged in her childrearing – but his presence in the home has been spotty and unpredictable. He often complains of the pressures of work, and is frequently gone from the home for business and social occasions. He faces unemployment at his job within the next two years. We can infer a lot of rubbish about Malia and Sasha Obama from our own bigoted mirror of race – but nothing about them as people.”
• Intimate partner violence (for women of reproductive age).
Wow, does this mean grandpa can’t be violent to grandma? Or gay men can’t be violent to their partners?
Another stupid socio-economic classification.
• Neighborhood median household income.
Who the hell knows that?
By the way, I liked your example of poor mixed-race Malia, Steve.
This is because you let them. Tell them no, I will not collect your data for you. I am a physician, not a social engineer. These people think they own you. You do too.
You want that meaningful use money or not? Do what you’re told, obey the golden rule.
Let’s stop and dwell on the most traditional lie on the list, race. What is that? Biologically, it is an utter fiction. Some say that it can be used for relative risk assignment for various genetic diseases which cluster in certain ways, based on some relatively tenuous statistics. But, as Steven Jay Gould wrote in “The Mismeasure of Man,” the term is based on a statistical fallacy – that continuous variables can be described in discrete categories that are arbitrarily assigned. A comprehension of the inner workings of the item studied need not be very advanced – simply the ability to separate “yes” and “no.”
Medicine has picked up the scientifically weak habit of calling 5% aggregate outliers of any statistic as “abnormal.” We forget that this calls our attention to something for the purpose of asking a question, not assigning an answer.
What does an ALT of 65 “mean?” In industrial clockwork medicine, it means a GI consult. It should rather draw one’s attention to hepatic cytolysis, and that it is somewhat elevated. Why is this? We are excused from thinking – simply putting things in primary colors is more convenient, if absolutely incorrect.
What are the principal races? Do Negro and Caucasian have meaning? Some “American Indigenous” tribes have been genetically separate for 10,000 years; what does that mean about “Native Americans?”
What of Jewish and Aryan? Many thousands of well-studied Europeans wrote reams and reams about these “races” and their characteristics – is Nazi race research intrinsically different than any other race research?
Some people say that it helps understand the social underpinnings of people by assigning them a race. What can we say about a mostly-Black, mixed-race girl who lives in government housing with her sister. Her mother has not been employed for most of her life. We know all about little Malia’s suffering. Her father has been engaged in her childrearing – but his presence in the home has been spotty and unpredictable. He often complains of the pressures of work, and is frequently gone from the home for business and social occasions. He faces unemployment at his job within the next two years. We can infer a lot of rubbish about Malia and Sasha Obama from our own bigoted mirror of race – but nothing about them as people.
We should have wiped out all the dreck and malignant dishonesty of racial classification when the Third Reich fell. Perpetuating of “race” in databases not only allows it to be considered by the wise who understand it’s complete absurdity – but by fools who believe there’s something true to it.
“Truth does not become more true by virtue of the fact that the entire world agrees with it, nor less so even if the whole world disagrees with it.” [perhaps the most honest physician in history]